Vicodin combines acetaminophen with hydrocodone—an addictive opioid—and many patients struggle with misuse and escalating tolerance.
This overview explains dependence and addiction cues, overdose danger, medically supervised cessation, and restorative treatment concepts.
What Is Vicodin?

Vicodin is a hydrocodone–acetaminophen combination FDA-indicated where non-opioid analgesics are inadequate.
- Hydrocodone (semi-synthetic) — see hydrocodone overview
- Acetaminophen adjunct potentiates analgesia but mandates liver exposure monitoring
Brand synonyms include combinations sold as Norco, Lorcet, etc.—follow exact pill imprint & prescriber instructions.
Side Effects
- Nausea, fatigue, sedation, constipation, headache, blurry vision—report severe reactions urgently
- Longer courses increase tolerance/overdose/organ-toxicity—including APAP hepatic insult
Combining Vicodin with other depressants (alcohol especially) synergizes respiratory inhibition.
Is Vicodin Addictive?
Hydrocodone products migrated to CSA Schedule II in 2014—mirroring potency & street demand.
- Escalating dose secretly or dissolving/snorting solids are abuse routes
- Psychological reinforcing effects stack with escalating tolerance
Vicodin Abuse Statistics

- NSDUH mis-use counts remain high for hydrocodone-containing products historically
- Poisoning deaths track multi-substance ingestion—never assume potency
Vicodin Addiction Signs and Symptoms
Physical
- Withdrawal on abrupt cessation (withdrawal primer)
- Lethargy, slurring, hypoventilation, cachexia/anorexia from chaotic use
Behavioral
- Secretive dosing, forging, doctor shopping when supply tightens
- Neglect domains of life/work despite consequences
Dependence versus Addiction
Tolerance/needing drug to baseline function contrasts with cravings & loss of control hallmarking addiction—overlap common.
Causes & Risks
Vicious neuroplastic loops from repeated dosing increase receptor count & dysphoria off-cycle—eventually even compliant therapy may stumble into physiologic reliance.
Unregulated street opioids escalate unpredictability exponentially.
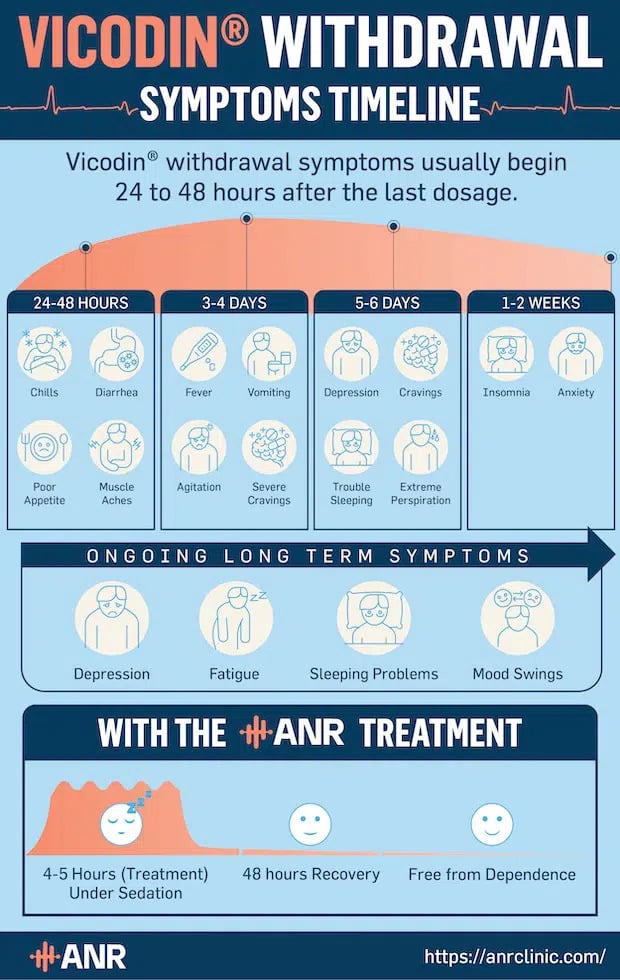
Withdrawal Symptoms
Consult Vicodin withdrawal; never stop high-dose alone—seizures, dehydration, suicidal ideation, relapse overdose.
Overdose
Pinpoint pupils, cyanosis, obtundation, seizure, vomiting—EMS + naloxone protocols; APAP hepatic necrosis unfolds on a different clock—coordinate emergency care urgently.
Relapse overdose risk escalates tolerance drops abruptly—paired with unknowable street purity.
Prevention Strategies
- Try multimodal/non-opioid analgesics first whenever feasible clinic-pathway allows
- Short-course lowest effective dose opioid when absolutely necessary—exit plan scripted
- Safe storage/disposal counseling
ANR Treatment

ANR addresses neuroendocrine perturbation underpinning relapse vulnerability—discuss suitability with admitting physicians—see full ANR description or request callback.
Key Takeaways
- Acetaminophen co-toxicity distinguishes combo pills from hydrocodone-only legacy mental models.
- Physical dependence emerges insidiously; psychological loss-of-control overlays later.
- Escalating without supervision threatens overdose—even “normal” relapse dose after abstinence may kill.
FAQ
1. Is Vicodin an opioid?
Yes—Vicodin contains hydrocodone, a potent semi-synthetic opioid; it is federally controlled.
2. What does Vicodin feel like?
People often describe relaxation and euphoria with pain relief; these rewarding effects elevate misuse risk even when taken as prescribed for some.
3. How quickly does Vicodin kick in?
Oral dosing commonly begins within tens of minutes, peaks roughly 1–2 hours, lasts on the order of hours—exact timing varies by formulation and metabolism.
4. How quickly does Vicodin kick in?
Oral dosing often produces effects within tens of minutes, peaks roughly 1–2 hours afterward, lasting several hours depending on formulation and metabolism.
5. Can I drink alcohol while taking Vicodin?
Do not combine without explicit medical clearance—risk of sedation, aspiration, hepatic strain (APAP metabolites), overdose.
6. Does Vicodin calm you down?
Sedating effects occur; misusing opioids for mood sedation outside medical indications increases dependence progression.
7. What options are available for treating opioid addiction in the U.S.?
Options vary by patient and severity—often including clinician-supervised stabilization, medication programs (sometimes called MAT), residential or outpatient rehab, behavioral therapies—and for appropriate candidates modalities like ANR. Review MAT context and how ANR is positioned with medical staff.
Additional Information